
Drug combinations and GBM
Drug combinations and GBM
Which repurposed drug combinations are most efficacious?

This is a big question and it is difficult to find an answer. We do have some useful information to draw upon however, as well as a few small studies.
One thing remains crystal clear in my mind. We urgently require new treatments and if we persist with the standard therapies we will continue seeing the standard response, which is not good. The development of new drugs is a lengthy process, often spanning several years, and their results are frequently underwhelming. Moreover, in the context of cancer, monotherapies are generally only partially effective, if effective at all.
How often do we hear about the latest ‘game changer’ or breakthrough’, only to be left disappointed? There is no magic pill. The only ones who benefit from this hyperbole are big pharmaceutical companies who profit off of these drugs.
Leveraging relatively cheap, repurposed, off-label drugs that target anomalies in cancer metabolism presents a promising strategy. However, in my view, to ensure the best outcomes, there should be increased support for patients to monitor progress and determine the most suitable drugs for their specific cancer.

I have seen first hand that this is a difficult thing to do on your own, especially if you are already feeling unwell or are simply apprehensive. You can of course see oncologists who are open minded, but too often this has to be done privately at places like the Care Oncology Clinic to have more open conversation. Many may not even realise this is a possibility, or patients could be thinking the first opinion they seek out should be the only path. I believe wider acceptance and support is vital, especially when patients have nothing to lose and their cancer is classed as incurable and/or terminal. There is great promise in repurposed drugs when time is taken to assess on a protocol that offers the most therapeutic benefit.
Repurposed (or ‘repositioned’ drugs) offer a number of key advantages.
Gliomas can easily develop resistance to standard treatments, off label drugs offer more options.
Using repurposed drugs, we can facilitate and accelerate the discovery of new cancer treatments.
In malignant glioma, like in other cancers, pre-existing physiological pathways that regulate cell growth, cell death or cell migration are dysregulated. We already have established, non toxic drugs that can target the metabolic derangement we see in cancer.
Recognition of these therapies would save a lot of time and money.
A comprehensive list of repurposed drugs that have been investigated in the literature for treating glioma can be found here in this review.
Some challenges remain.
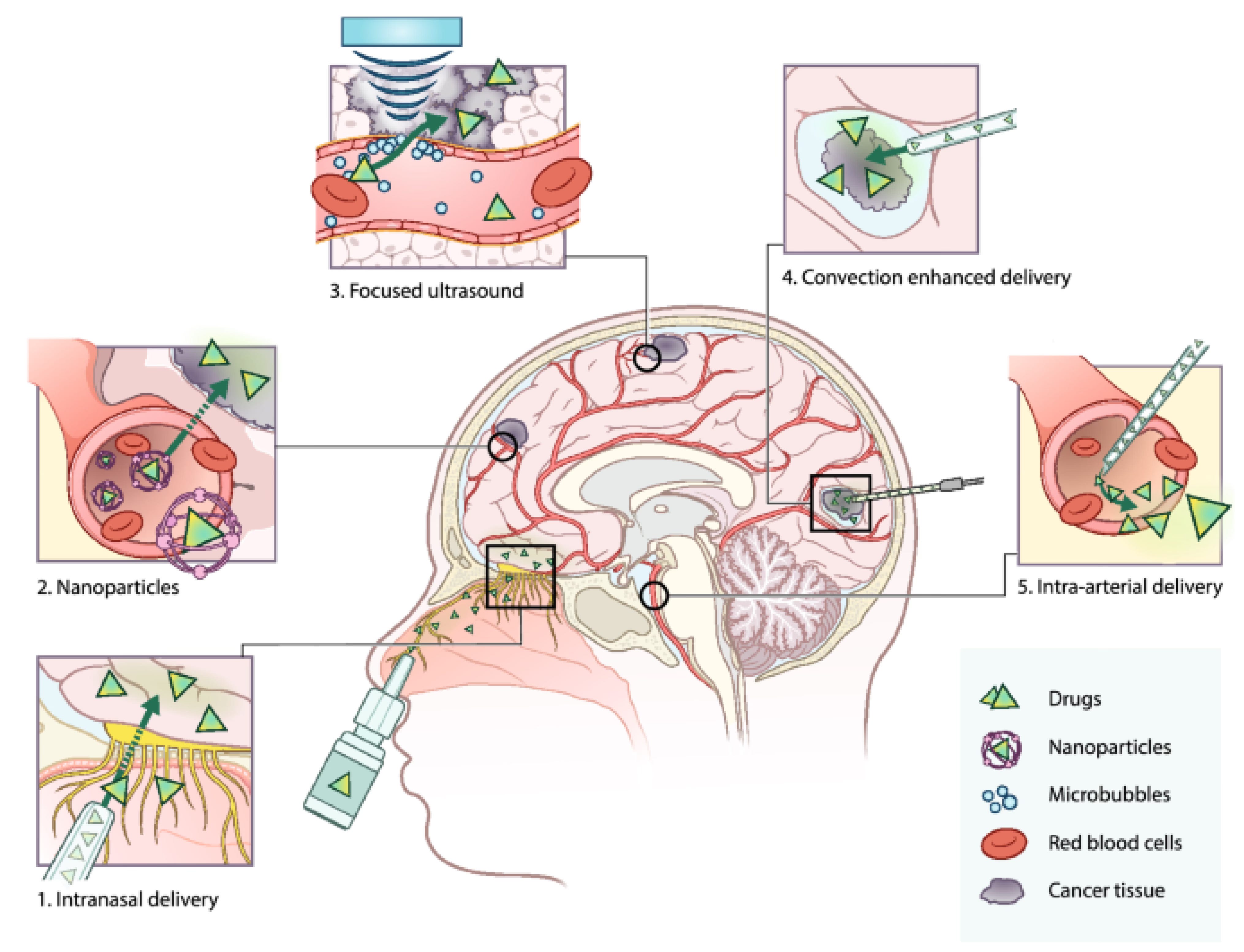
Notoriously, one notable obstacle to getting drugs to the brain at therapeutic doses is the blood brain barrier. Patients must be aware of how much of these repurposed drugs are required to achieve a beneficial response without undesirable side effects. There has been some progress in looking at novel routes of administration of these drugs, as shown in the graphic below.
Personally I really like the idea of intranasal delivery, particularly as I realise brain tumours can actually be caused by inhaling volatile compounds, such as vinyl chloride, trichloroethylene and certain ‘forever chemicals’ like ‘Per and polyfluoroalkyl substances (PFAS)’, so it makes sense that we could have compounds that can be used to treat cancer via this route of administration.
I know many people who have done this now (drug repositioning), with mixed results. Some extraordinary, some disappointing.
To ensure success, I think a key question should be - do you want to follow a scatter gun approach with lots of different drugs? … or do you want to just focus on a few drugs with a methodology that is more refined? Each approach has pros and cons. Personally I’m drawn to the more refined approach.
Key considerations. What I personally think is most important to look at:
Keep reading with a 7-day free trial
Subscribe to Andrew’s Substack to keep reading this post and get 7 days of free access to the full post archives.