

Is it the hope that kills you?
Examining the efficacy of the standard of care for brain cancer

For this analysis I will be looking specifically at the standard of care for high grade glioma, which consists of surgery, chemotherapy and radiotherapy. Of course if surgery is a viable option, the benefits will most likely outweigh the risks in most cases, but how robust is the evidence supporting the use of chemotherapy (in the form of tomozolomide) and radiotherapy for this kind of cancer?
The most common chemotherapy and radiotherapy protocol for glioblastoma is the Stupp protocol, which is named after Dr. Roger Stupp, who led the clinical trial that established this treatment approach. It was said to be a ‘landmark study’, that changed the way we treat high grade glioma brain tumours.
The Stupp protocol involves the following steps:
Surgery: The primary goal is to remove as much of the tumor as possible without causing significant damage to the surrounding brain tissue.
Concurrent chemoradiation: After surgery, patients typically undergo a combination of chemotherapy and radiation therapy. The chemotherapy drug most commonly used is temozolomide (TMZ). During this phase, patients receive radiation therapy (usually external beam radiation) five days a week for approximately six weeks, along with daily oral temozolomide.
Adjuvant chemotherapy: Following the concurrent chemoradiation phase, patients receive adjuvant chemotherapy with temozolomide. This usually involves taking the drug for five days during each 28-day cycle, for a total of six cycles or until the tumour progresses.
What is the rationale for supporting this approach?
Most researchers will argue that The Stupp protocol has become the standard of care for newly diagnosed glioblastoma patients because it has been shown to improve overall survival compared to radiation therapy alone. Within the protocol, each patient's treatment plan may be adjusted based on factors such as age, overall health, and tumor characteristics, though the main principles remain the same. The main differences are likely to be strength of radiation and considerations relating to the Karnofsky Performance Score (KPS), a quality of life and general function metric indicating how well patients are able to tolerate chemotherapy.
Let’s take a deeper dive into the study methodology to assess how reliable the results are.
It's important to point out that in the context of this investigation, there is no control group receiving no treatment, as this would be considered unethical. This makes it challenging to fully evaluate the benefit at a time when surgical, pharmacological, and imaging techniques have become highly advanced. The survival data gathered before the advent of radiotherapy is derived from an era when surgical and imaging techniques were less sophisticated, likely leading to inferior outcomes. Therefore, it would be challenging to accurately measure how survival outcomes might have compared with the technology we have at our disposal today.
In this study, the 'control' group comprises individuals receiving only radiotherapy, while the treatment group includes those treated with both radiotherapy and temozolomide.
I appreciate that this type topic can be a heavy subject to approach, so let’s attempt to break down the main points, with graphics:
What is the Stupp Protocol?
The Stupp protocol combines temozolomide (TMZ) chemotherapy with radiation therapy.


The landmark study that established the protocol was published in the New England Journal of Medicine in 2005 and changed the way we treat malignant brain tumours.
What was the methodology?
Trial duration: August 2000 - March 2002
Total patients: 573
Randomised groups:
Radiotherapy (286 patients)
Radiotherapy + Temozolomide (287 patients)
Patient characteristics:
Median age: 56 years
Surgical intervention: 86% of patients had debulking surgery.

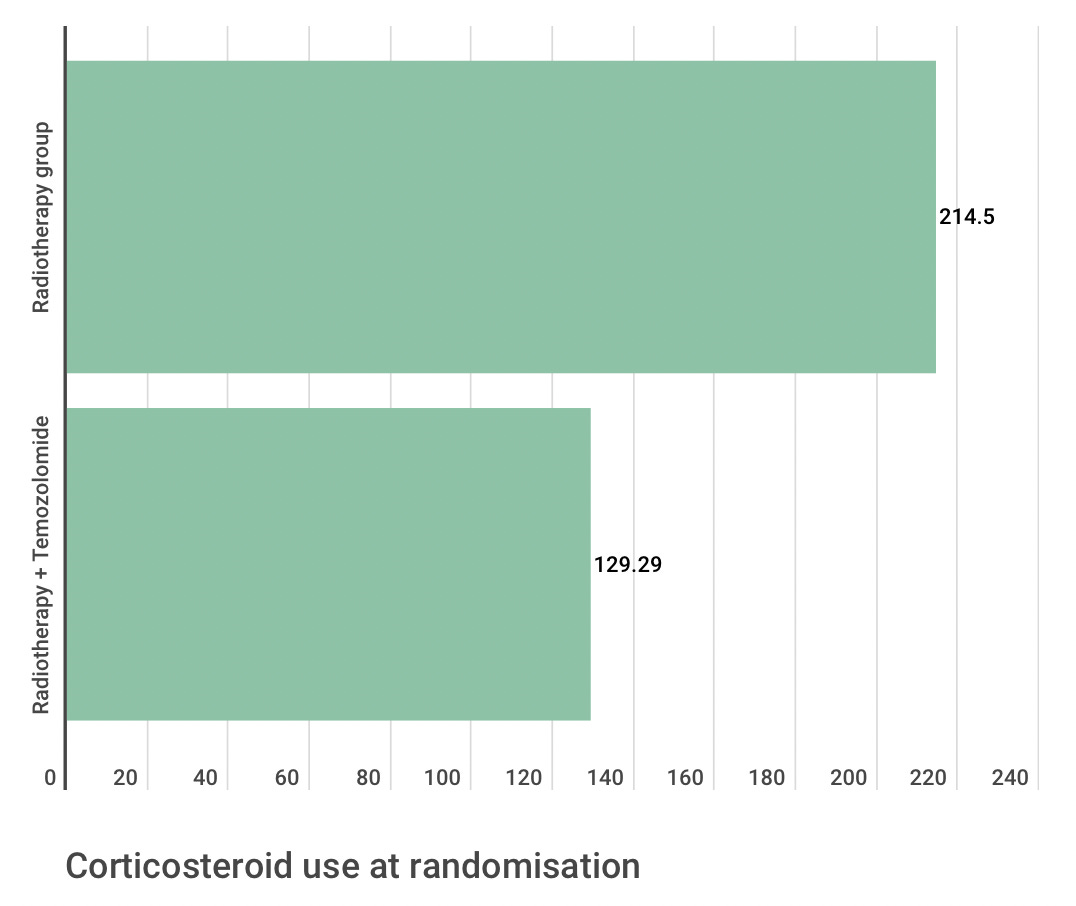
Corticosteroid use at randomisation:
Radiotherapy group: 75%
Radiotherapy + Temozolomide: 67%
Central pathological review:

Median follow up (28 months):
480 patients (84%) had died
Median survival benefit: 2.5 months
Radiotherapy plus temozolomide - 14.6 months
Radiotherapy alone - 12.1 months
Median progression-free survival:
Radiotherapy plus temozolomide - 6.9 months
Radiotherapy alone - 5 months
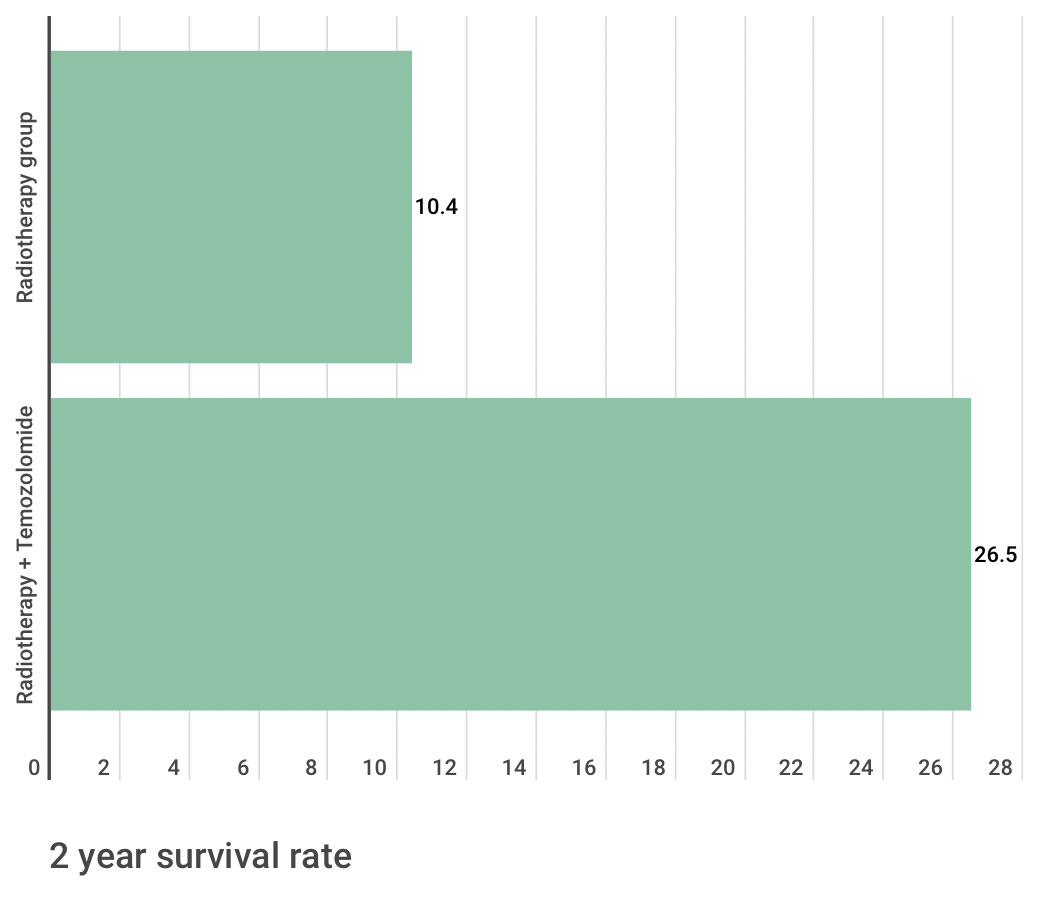
Two year survival rate:
Radiotherapy plus temozolomide - 26.5%
Radiotherapy alone - 10.4%
Improved median overall survival with radiotherapy plus temozolomide in most subgroups apart from a subgroup of 93 patients who underwent biopsy only and 70 patients with poor performance status.
What do we make of the results?
The results may not be as clear as one might presume at first glance due to a number of factors and so I would argue that more strict inclusion characteristics could draw more reliable results. With that being said, I understand that it is very difficult to not have confounding variables with this patient population at the numbers seen in the trial and I am not completely discrediting the data we have.
As stated, patients who received the combination of temozolomide and radiation therapy had a median overall survival of 14.6 months, compared to 12.1 months for patients who received radiation therapy alone. The two-year survival rate was also higher for patients who received the combined treatment (26.5%) compared to those who received radiation therapy alone (10.4%).
In an ideal world, conditions of the trial would be more consistent. We know that in the ‘control’ group (radiation alone), there were a greater number of patients on corticosteroids. This may have had an impact of progression free and overall survival so you would either want to have the same number of patients on corticosteroids in both groups. The groupings themselves has the potential to bring down the average survival in one group as opposed to the other.

One factor that was not taken into account in the original trial was MGMT status. Ideally you would want conditions to be as close in both groups as possible, with only the treatment being different, and so in retrospect this can be seen as a flaw in more recent research that as far as I could tell hasn’t replicated a robust trial under conditions taking into account molecular characteristics. It has absolutely been mentioned, and there is reliable survival data, but not at the same level. We know that the timing of temozolomide administration likely makes little to know difference to overall survival, which is good to know, but for me the overall data leaves more questions than answers that have yet to be fully investigated, especially in light of what we know now. Even on this topic there are contradictory reports, with morning often appearing to show a greater degree of benefit in this retrospective study, as well as mechanistically, exerting its effect more potently through interaction with clock genes and circadian biology.
Keep reading with a 7-day free trial
Subscribe to Andrew’s Substack to keep reading this post and get 7 days of free access to the full post archives.